





























Introduction: Understanding Bone Grafting Limitations
Not all patients possess the adequate bone volume necessary for the successful placement of dental implants. This issue is particularly common in the posterior maxilla, especially beneath the maxillary sinus. While patients with significant bone atrophy may be ideal candidates for bone augmentation procedures—essentially the only reasonable method to provide them with fixed restoration—debate exists regarding the treatment of patients with “moderate” bone levels. Generally, three primary concerns arise with bone augmentation surgeries: the associated costs and duration of treatment, heightened patient discomfort, and unpredictable success rates. As a result, contemporary clinical studies increasingly focus on evaluating the performance of shorter implants (5-8 mm) or angled implants, either in conjunction with or independent of less invasive bone augmentation techniques.
The Potential of Alveolar Ridge Augmentation
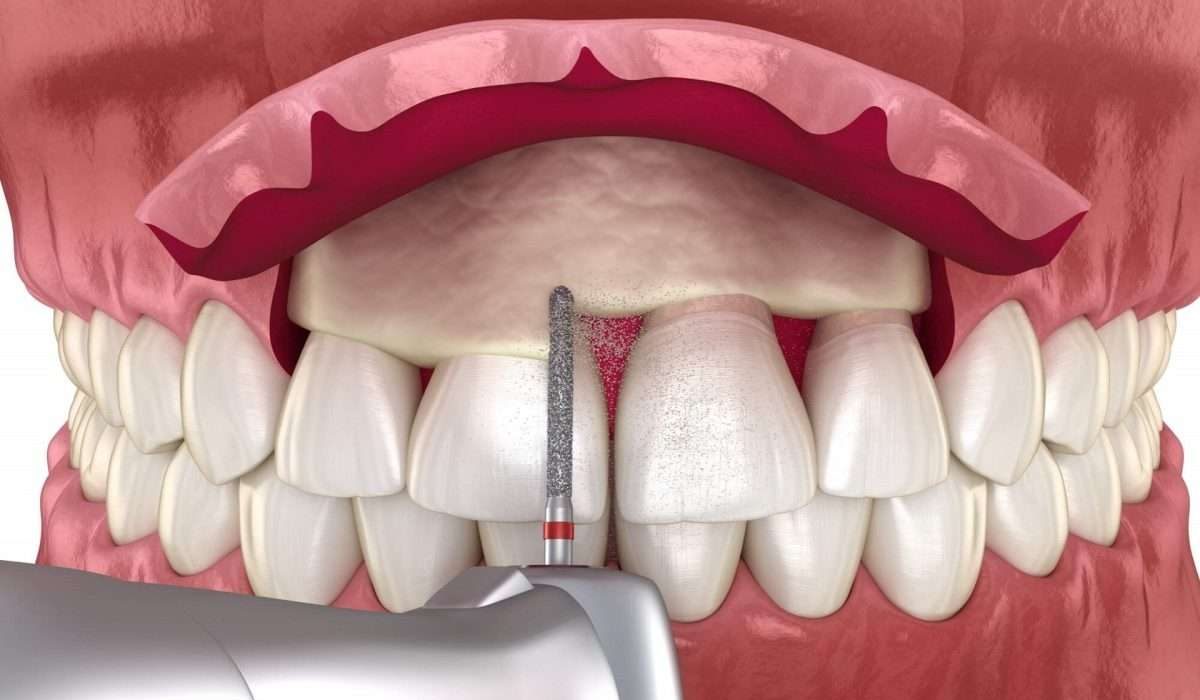
In moderately atrophic posterior maxillae (remaining bone height of 3-6 mm), the use of the alveolar ridge approach for sinus lifting may represent a less traumatic alternative to conventional lateral wall sinus elevation techniques. The lateral window technique for sinus elevation is one of the most commonly employed bone augmentation procedures and is regarded as a reliable surgical method, particularly when using autogenous bone. This approach, originally reported in the late 1970s, involves the careful elevation of the sinus membrane after creating a window in the lateral wall of the maxillary sinus, with autogenous bone (or bone substitutes) placed within the sinus to heal for approximately six months or longer before implant placement. Variations of this technique, with minor modifications, are still widely practiced today.
Innovations in Sinus Lift Techniques
The simultaneous placement of implants during sinus elevation can significantly reduce the reconstruction time if there is sufficient bone to stabilize the implants. To further minimize patient discomfort, a technique was proposed to elevate the sinus directly from the implant site via the alveolar ridge. Initially described by Tatum in 1986 and later modified by Summers in 1994, this approach contrasts the lateral window technique by elevating the sinus membrane with a bone elevator and subsequently placing the implant into the prepared site. Cosci further refined this alveolar ridge method by introducing a range of different length drills, including a non-traumatic elevating drill, to minimize the risk of sinus membrane perforation. Bone can also be harvested directly from the ridge and used as grafting material.
Despite the reduced invasiveness of the ridge approach, some disadvantages persist. The bone volume attainable through the ridge access is typically less than what can be harvested using the lateral wall technique. Moreover, a minimum ridge height of approximately 3 mm is generally required to stabilize the implant at the time of placement. Consequently, shorter implants are often needed for procedures involving alveolar ridge elevation. Conventionally, implants measuring 8 mm or shorter are thought to lack reliable long-term outcomes. A review of available literature indicates that the failure rate for 7 mm implants is around 10%. While these data must be interpreted cautiously, as they may reflect severe underestimations due to poor research quality, they still suggest that shorter implants may have inferior prognoses compared to longer implants. This perspective is prevalent among dentists, who tend to favor the placement of implants that are at least 10 mm long. When sufficient bone exists to accommodate longer implants, this strategy is clinically sound; however, dentists often face a dilemma between utilizing 5-8 mm short implants or opting for bone augmentation to place longer ones.
The Healing Process and Early Loading Potential of Implants
Implants placed within the augmented maxillary sinus typically require a healing period of at least four months, and more commonly longer, to allow for the formation of new bone prior to functional loading. Data suggest that early loading of implants in non-grafted sites can be quite successful when performed by experienced clinicians. The potential for a minimally invasive technique that employs an 8 mm short implant for enhancing the residual bone height of 3 to 6 mm through sinus elevation presents an exciting opportunity. Exploring whether this method can shorten the non-loading period for implants could provide significant benefits to patients.
Materials and Methods: A Comparative Study
In our study, we sought to compare the effects of placing long implants (10-16 mm) following bone grafting via the lateral wall approach against the use of short implants (8 mm) following grafting via the alveolar ridge top approach. We enrolled 40 partially or totally edentulous patients with residual alveolar ridge heights of 3-6 mm and a minimum maxillary sinus floor thickness of 4 mm, randomly assigned to two groups based on a parallel-group design. One group received grafting with a 50% mixture of inorganic bovine bone (Bio-Oss®) and 50% autogenous bone, followed by the implantation of 1 to 3 hydroxyapatite-coated implants measuring 10 to 16 mm (20 patients). The contrasting group underwent grafting with autogenous bone via the alveolar ridge approach and received 8 mm implants (20 patients).

After a healing period of 45 days, implants were submerged and subsequently loaded with a screw-retained temporary prosthesis made of all-acrylic within a week of abutment connection. After 45 days, temporary cemented final metal-ceramic restorations were placed. Outcome measures included failures of the prosthesis or implants, complications, and radiographic changes in the marginal bone level around the implants. Moreover, the stability of individual implants was assessed blindly at baseline, as well as one and five years post-loading, utilizing Osstell® and Periotest.
Results: Implant Performance and Complications
During the study, one patient withdrew from the long implant group due to death. In the short implant group, one implant failed, while in the longer implant group, five implants failed across three patients, a difference that lacked statistical significance. Four patients in the short implant group experienced four complications, whereas seven patients in the long implant group encountered eight complications; again, this difference was not statistically significant. Notably, two significant postoperative complications occurred within the long implant group: one case of an abscess and another of sinusitis, leading to treatment failure in two patients (involving four implant losses).
Five years post-placement, the mean marginal bone loss was recorded at 0.72 mm for long implants and 0.41 mm for short implants, with this difference reaching statistical significance (P = 0.028). Over time, Osstell® values demonstrated an increase while Periotest scores decreased, with no differences noted between the two groups at any time point.
Conclusion: A Favorable Approach for Moderate Atrophy
In conclusion, for patients presenting with a residual bone height of 3 to 6 mm in the atrophic posterior maxilla, the placement of 8 mm short implants following alveolar ridge augmentation could be a more favorable option compared to the placement of longer implants following lateral wall sinus elevation. This technique minimizes patient discomfort and offers an effective alternative. If these implants are inserted with an implant torque exceeding 35 Ncm, and connected to the same prosthetic restoration, they may allow for early loading as soon as six weeks post-surgery.
Conflict of Interest Statement
This study was entirely self-funded and did not receive any commercial support, including materials provided free of charge.












{kind=link}
Discussion about this post